Every surgical procedure depends on what happens before the first incision. The sterile processing department is where surgical instruments are cleaned, sterilized, tracked, and stored — and where compliance failures become patient safety events. Four regulatory bodies set the standards: HSPA, AORN, AAMI, and the Joint Commission. Each targets a different layer of SPD operations. Together, they define what safe, compliant sterile processing looks like — and what's at stake when facilities fall short.
Key Takeaways
SPD compliance is the set of standards and regulations that govern how a sterile processing department cleans, sterilizes, stores, and tracks medical and surgical instrumentation. When these standards are met, surgical facilities can deliver quality care. When they aren't, the consequences reach directly into the operating room.
SPD compliance is infection prevention in practice. Research by Nichol et al. (2024) found that 26.16% of surgical cases experienced at least one instrument error — making poor compliance a measurable patient safety threat, not a theoretical one. SPD-related delays cost a single facility between $6.75M and $9.42M annually in lost chargeable OR minutes. Scaled across the U.S. healthcare system, that figure becomes a multi-billion-dollar burden.
The risk is direct: any medical device that hasn't been properly sterilized is a potential vector for surgical site infection — even if it looks clean.
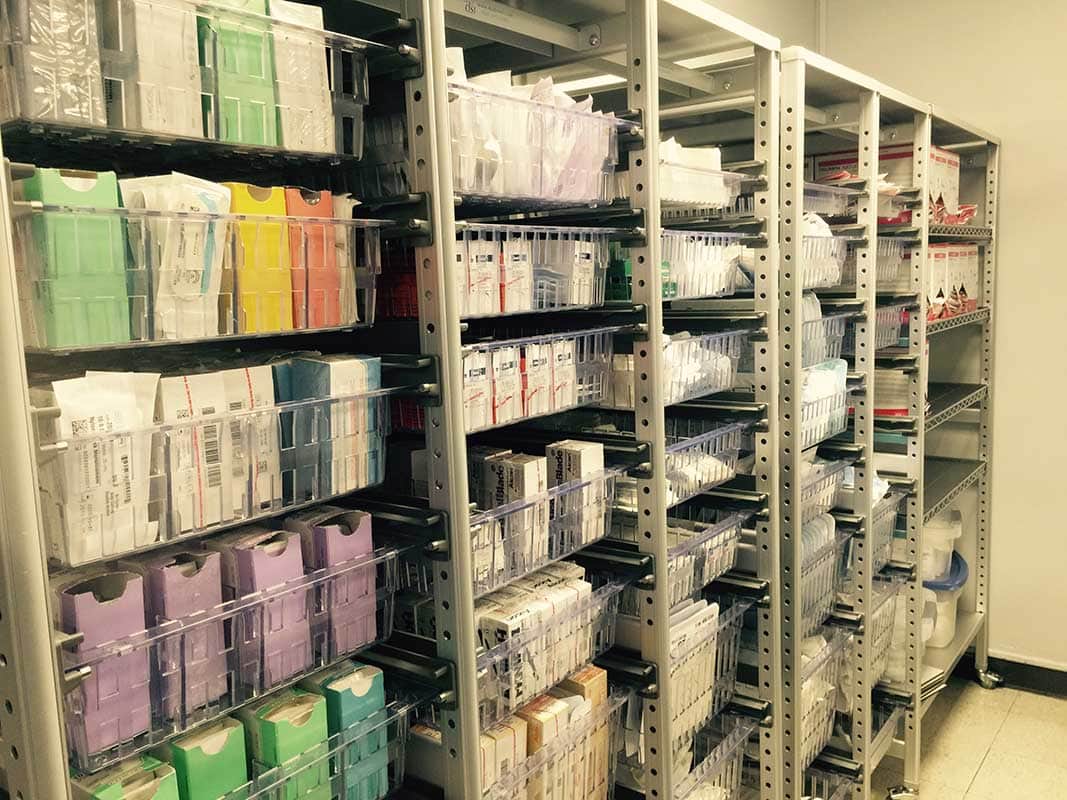
Sterile storage is where compliance either holds or breaks down. The Joint Commission consistently identifies sterile storage deficiencies as among the most common infection control findings during accreditation surveys. The most cited issues: instruments stored on the floor, uncontrolled temperature and humidity, overstuffed shelves that damage packaging integrity, and sterile items mixed with non-sterile ones.
Per AAMI ST79, a surgical instrumentation set that has been perfectly cleaned, packaged, and sterilized can still become a patient safety risk if stored improperly. Sterile processing workflows and sterile instrument storage are inseparable — best practices in one cannot compensate for failures in the other.
Four bodies set the rules for sterile processing department operations. Each regulates a distinct layer — education, clinical practice, technical standards, and accreditation — and together they define what full SPD compliance looks like.
HSPA's Sterile Processing Technical Manual (9th ed., 2023) is the field's definitive reference. It covers decontamination, sterilization methods, packaging, sterile instrument storage, instrument management, and quality systems. HSPA also administers four certifications: CRCST (technicians), CIS (instrument specialists), CHL (managers), and CER (endoscope reprocessors). New Jersey, New York, and Tennessee have already moved toward mandating CRCST certification — a clear signal that credentialed staffing is becoming a regulatory floor, not a best practice.
AORN's Guidelines for Perioperative Practice are updated annually. The 2023 edition added guidance for sterilizing 3D-printed medical devices, clarified safe use of abbreviated sterilization cycles (IUSS), strengthened transport requirements for sterilized items, and aligned explicitly with AAMI ST108 water quality standards. Both AAMI ST79 and AORN also require a minimum 24-hour notice for loaner instrument sets — late arrivals are one of the most common compliance breakdowns in surgical facilities.
AAMI standards use precise language: "shall" means required, "should" means recommended. ANSI/AAMI ST79 is the most referenced SPD standard, governing everything from facility design to sterilization cycles. ST108:2023 adds water quality requirements at every reprocessing stage.
The Joint Commission accredits more than 22,000 U.S. healthcare organizations — and accreditation affects Medicare and Medicaid reimbursement. SPD is evaluated across five chapters: Environment of Care, Infection Prevention, Leadership, Human Resources, and Performance Improvement. The most cited deficiencies: not following manufacturer IFUs, incomplete sterilization documentation, improper sterile storage, and insufficient staff competency verification.
Meeting all four sets of criteria comes down to two things: disciplined workflow execution and a physical environment built to spec. Neither alone is enough.
Sterilization monitoring runs on a hierarchy. Biological Indicators (BIs) sit at the top — they use Geobacillus stearothermophilus spores to directly measure sterilization lethality. Per AAMI ST79, a process challenge device (PCD) with a BI must run at least weekly, preferably daily. Every implant load requires one, and that load stays quarantined until results are confirmed. Below BIs, Chemical Indicators (CIs) provide package-level verification. ANSI/AAMI/ISO 11140-1 defines six CI types, from basic process indicators (Type 1) to integrating indicators (Type 5) that match BI-level performance.
Workflow design matters just as much as monitoring. AAMI ST79 mandates a unidirectional flow from soiled to clean — no crossover, ever. Physical barriers between decontamination and prep/packaging areas are strongly recommended. Internal audits must occur at least quarterly to catch gaps before surveyors do.
Every SPD zone has defined environmental requirements under AAMI ST79 and FGI Guidelines:
| Zone | Pressure | ACH | Temp | RH |
| Decontamination | Negative | ≥10 | 60–65°F | 30–60% |
| Prep/Packaging | Positive | ≥10 | 68–73°F | 30–60% |
| Sterilization | Positive | ≥10 | 68–73°F | 30–60% |
| Sterile Storage | Positive | ≥4 | 65–75°F | 30–60% |
Shelf clearance is non-negotiable: 8–10 inches off the floor, 18 inches from the ceiling, 2 inches from exterior walls. Stock rotates FIFO. And sterility is event-related — an item is sterile until its packaging is compromised, not until a date passes.
Compliance audits don't just check policies — they trace actual workflows and examine real records. Surveyors look for evidence that standards are being followed consistently, not just documented on paper.
Documentation is audited at the cycle level. AAMI ST79 and the Joint Commission require complete records for every sterilization run: sterilizer ID, cycle parameters, load contents, physical/chemical/biological monitoring results, and the operator's name. Records must be retained long enough to support a full recall if a sterilization failure is later identified.
Handling is equally scrutinized — and the data shows why. Nichol et al. (2024) found that 88.6% of all instrument errors stem from failures in visualization tasks: inspection, identification, and function assessment during sterile processing. The most common errors found in audits are missing instruments (160 instances), broken or poorly functioning instruments (44 instances), and tray assembly errors (13 instances). These aren't documentation failures — they're hands-on process failures that auditors can identify directly.
The Joint Commission uses tracer methodology. Surveyors follow a single contaminated instrument from OR return through decontamination, inspection, assembly, packaging, sterilization, and storage. This approach surfaces systemic gaps that a policy review would never catch. Facilities offering off-site centralized sterile processing are also evaluated under the CSS (Centralized Sterilization Services) Certification, which adds scrutiny of interfacility transport protocols and multi-site regulatory adherence.
To stay audit-ready year-round, performance improvement programs should track five core KPIs: biological indicator failure rates, wet pack rates, instrument error rates, sterilization cycle documentation completeness, and turnaround time (TAT).
Long-term compliance isn't sustained by audits alone — it's built into daily operations through standardized procedures, measurable benchmarks, and infrastructure that supports consistent performance.
Benchmarks give compliance a measurable baseline. High-performing SPDs target: instrument tray accuracy ≥98%, OR first-case on-time starts ≥90%, turnaround time ≤4 hours (≤2 hours for priority sets), instrument error rate ≤2 per 100 cases, and staff satisfaction ≥8/10.
Technology enforces those benchmarks at scale. RFID tracking automatically logs sterilizer entry and exit, flags unprocessed sets, and locates instruments within the storage system — creating a continuous digital audit trail. Barcode scanning achieves similar documentation at a lower cost. Environmental monitoring systems watch temperature, humidity, and air pressure in sterile storage areas in real time, triggering alerts before conditions can compromise sterile items.
The case examples are instructive. A 350-bed community hospital facing multiple Joint Commission citations installed high-density mobile shelving — increasing storage capacity by 35% while maintaining full AAMI ST79 compliance. The follow-up Joint Commission visit produced zero citations, and the facility subsequently earned full HSPA certification for its SPD program.
A newly built 8-OR ambulatory surgery center integrated RFID tracking from day one, saving an estimated 45 minutes per day in instrument location time. It passed initial Joint Commission accreditation with zero sterile storage or infection control citations, and the full storage investment paid for itself within the first year.
One consistent lesson: high-density mobile shelving requires a floor load assessment and infection control review before installation. The most cost-effective window is during facility design or renovation — retrofitting is significantly more disruptive and expensive.
SPD compliance isn't just a regulatory checkbox — it's a direct driver of clinical and operational performance. The data connecting service quality to patient outcomes is clear and consistent.
The gap between high- and low-performing SPDs is measurable. Facilities rated excellent in SPD service quality achieve a patient safety incident rate of 0.9‰ — compared to 8.5‰ for poor-service facilities. That's nearly a 9-fold difference. Compliance audit scores reflect the same divide: 94/100 for excellent facilities vs. 58/100 for poor ones.
Operational results follow the same pattern. A large academic medical center with 42 operating rooms implemented a structured SPD–OR improvement program — daily coordination huddles, a shared instrument tracking dashboard, joint quality meetings, and cross-training. SPD-related first-case delays dropped from 8.8% to 2.1% in 12 months.
The performance gap between excellent and poor SPD service is stark across every metric. Instrument error rates: 3.2% vs. 26.2%. OR case delay rates: 2.8% vs. 22.0%. Each percentage point represents chargeable OR minutes, physician satisfaction, and patient outcomes.
Staff satisfaction follows the same curve: 9.4/10 at excellent-service facilities vs. 4.2/10 at poor ones — making infrastructure investment a retention strategy as much as a compliance one.
The 42-OR academic medical center entered its improvement initiative with a 22% first-case delay rate, SPD issues driving roughly 40% of those delays. After the intervention, OR staff satisfaction with SPD services rose from 4.8 to 8.3/10. SPD staff satisfaction climbed from 5.2 to 7.9/10. Compliance investment paid off operationally and culturally.
Distribution Systems International has specialized exclusively in healthcare storage since 1990 — over 30 years serving acute care facilities across all 50 states. DSI doesn’t sell general commercial shelving; every product and service is designed specifically for SPD, OR, and materials management environments. The DSI process is consultative from the start: on-site analysis, CAD-designed layouts, ROI calculations, full turnkey installation, and ongoing after-sales support. That end-to-end accountability is what separates DSI from vendors who deliver a product and move on.
Choose DSI if:
Distribution Systems International has partnered with acute care facilities for over 30 years to design, implement, and optimize sterile instrument storage systems built to AAMI, AORN, and Joint Commission standards. Whether you're preparing for an accreditation survey, addressing cited deficiencies, or building a new SPD from the ground up, DSI delivers turnkey solutions that close compliance gaps and protect patient safety. Contact Distribution Systems International today to schedule a complimentary storage analysis.

With 21 years of sales management, marketing, P&L responsibility, business development, national account, and channel management responsibilities under his belt, Ian has established himself as a high achiever across multiple business functions. Ian was part of a small team who started a new business unit for Stanley Black & Decker in Asia from Y10’ to Y14’. He lived in Shanghai, China for two years, then continued to commercialize and scale the business throughout the Asia Pacific and Middle East regions for another two years (4 years of International experience). Ian played college football at the University of Colorado from 96’ to 00’. His core skills sets include; drive, strong work ethic, team player, a builder mentality with high energy, motivator with the passion, purpose, and a track record to prove it.